David Rasnick
The AIDS
Ribbon is a Noose Around the Neck of Africa
Dedicated to the memory
of
my friend and great Zulu warrior,
Professor Sam Mhlongo.
As of May 7,
2008, there were 440 clinical trials underway in South Africa. Ten were
evaluating Atazanavir, Efavirenz, Tenofovir,
and Acyclovir in combination with
different toxic anti-retroviral drugs (known as HAART) in HIV-positive people (Department
of Health, 2008). In
2005, the Dr. Rath Health Foundation Africa (a not-for-profit organization)
contracted with my friend Professor Sam Mhlongo, Head of Family Practice at the
Medical University of Southern Africa (MEDUNSA), to sponsor a clinical trial
titled “Vitamins in HIV-positive patients”. The clinical trial was a
professionally designed double-blind, placebo-controlled, randomized study of
the value of nutritional supplements in preventing and reversing the various
diseases known as AIDS in Africa. I was asked to setup and run the analysis lab
that would support the clinical trial. We spent almost two years trying to get
the nutritional clinical trial approved.
President Thabo
Mbeki’s political enemies along with the AIDS mainstream prevented this trial
from taking place. Professor du Plooy
of MEDUNSA led the attack. Below is the formal complaint we sent the Department
of Health regarding Professor du Plooy’s
opposition to our study.
----------------
Complaints
against Professor du Plooy
By
David Rasnick, PhD and Professor Sam Mhlongo, MD
Dec.
2005
1.
We
accuse Professor du Plooy,
chairman of the ethics committed, of bias against the Dr. Rath Health
Foundation, Dr. Rath personally, Professor Mhlongo and Dr. Rasnick. This bias
is manifest in du Plooy’s
public statements and leaking information to the Democratic Alliance, Treatment
Action Campaign, and Medicines Control Council.
2.
We
accuse du Plooy of
systemically blocking the ethics committee approval of our micronutrient
clinical trial at MEDUNSA.
3.
Professor
du Plooy’s blocking of the
micronutrient clinical trial has kept crucial information from the people of
South African on the natural approach to health.
4.
Professor
du Plooy’s blocking of the
micronutrient clinical trial has cost the Dr. Rath Health Foundation
considerable time and money that could have been devoted to helping the people
of South Africa.
Professor du Plooy’s ever-changing requirements for ethics committee
approval are a moving target. The fact that he brings up bogus objections at
the eleventh hour, after more than a year of review reflects a definite effort
to delay indefinitely the start of our clinical trial.
Professor
du Plooy is a member of the
secret Medicines Control Council, which has experienced considerable pressure
from the DA (opposition party of which du Plooy is a member), the Treatment Action Campaign, and the
South African Medical Association to halt any and all investigations by the Dr.
Rath Health Foundation into the health benefits of micronutrients in the
context of AIDS in South Africa.
On October 13,
2005, Professor du Plooy
justified his rejection of our proposed clinical trial in an interview with Health-e: “In this case, MCC approval
has not been submitted to us yet. We normally look out for, in the protocol,
whether it should get MCC approval or not. And this one should get MCC
approval.”
Professor du Plooy shared with the
interviewer that the committee raised over 34 concerns with the protocol,
implying major problems. Almost all of those 34 concerns were pointing out
typographical errors. The substantive issues were: 1) better Tswana translation
of patient information leaflet, and 2) proof of insurance for the study.
All of the ethics committee’s “34 concerns” of
May 5, 2005, were completely dealt with months before the Professor’s interview
with Health-e on Oct. 13.
Specifically:
a. All typos were corrected as suggested.
b. The Tswana version was completely
re-translated and checked by two independent readers fluent in Tswana. Both
readers said that the Tswana translation was a fair and accurate representation
of the corrected English version.
c. Also, we provided proof that we had purchased
insurance coverage for the doctors and patients in the study.
Professor du Plooy’s assertion that our
proposed micronutrient clinical trial should have MCC approval is disingenuous,
at best. There is no reason for MCC approval because our trial involves only
micronutrients, not pharmaceutical drugs or medical devices. Micronutrients do
not come under the purview of the MCC.
Further along
in the same Health-e interview,
Professor du Plooy confuses
the nutritional programs in Khayelitsha with the
proposed micronutrient clinical trial under review at MEDUNSA, saying: “It’s an
unethical trial.” There is nothing unethical about the nutritional programs in Khayelitsha, which have nothing to do with the proposed
MEDUNSA clinical trial.
The nutritional
programs in Khayelitsha are organized and conducted
under the auspices of SANCO. The Dr. Rath Health Foundation provides SANCO with
micronutrients free-of-charge. The nutritional programs use licensed South
African physicians to monitor the health of individuals and give the
micronutrients to them at no charge. It is certainly well-within
the law for licensed physicians to provide vitamins and other micronutrients to
people.
The Annex 2 of Prof W J du
Plooy is complete nonsense, clearly instigated by
outside forces intent on killing our clinical trial. The formulations used in
the trial are not for supplementing the diets of healthy people. They are test
formulations proved in Europe and elsewhere and deemed necessary by the
principal investigator for the study. This is standard practice in all clinical
trials. The fact that du Plooy
brings up this bogus objection at the eleventh hour, after more than a year of
review, indicates a definite effort to delay indefinitely the start of our clinical
trial.
----------------
At President Mbeki’s instruction, Health
Minister Manto met with us to discuss how best deal with Professor du Plooy’s attacks on our
proposed clinical trial. The Minister agreed to contact du
Plooy directly and resolve the problem. Regrettably,
this didn’t happen.
The first week of January 2006, Sam and I went to talk with President Mbeki about this. Sam was allowed over one hour with the president. However Essop Pahad, Minister to the President, advised Mbeki not to see me. He told Mbeki it would be politically bad if it were leaked that the president had spoken with an employee of the Dr. Rath Health Foundation. The President told Sam he wished he could have met with me and that he privately supports the work of the Foundation but there can be no direct link with its activities.
Faced with the inability to get approval for our nutritional clinical trial, I left South Africa July 2006. Sadly, in October 2006, my friend Sam Mhlongo was killed in a traffic accident. The following is the story of what we were able to accomplish in spite of the mean-spirited and relentless opposition to our efforts.
To
understand AIDS in Africa one needs only to understand the African context.
“I was in Malawi and met with
a group of women living with HIV. As I always do when I meet people with
HIV/AIDS and other community groups, I asked them what their highest priority
was. Their answer was clear and unanimous: food. Not care, not drugs for
treatment, not relief from stigma, but food.”
Peter Piot, UNAIDS Executive Director (Piot, 2003)
Sam continually
asks, Where do you find AIDS in Africa? In the affluent areas of Cape Town, Durban, and Johannesburg?
or across the bay from Cape Town in Khayelitsha township? Or north of
Pretoria in Soshanguve township? or the countless shantytowns without names where tens of
millions of desperately poor black South Africans live?
In the
1950s, the United Nations and its agencies became involved in evaluating the
extent of profound malnutrition worldwide. Since then, considerable resources
have been directed towards improving the treatment of those suffering from this
serious and complicated condition. Tragically, however, the fatality rate for
severe malnutrition has remained unchanged over the past five decades (Schofield
and Ashworth, 1996).
The growing gap between nutritional knowledge
and practice in the developing world led
Alan Berg of the World Bank in 1993 to accuse nutritionists and pediatricians
of malpractice for failing to improve nutrition in the developing world despite
considerable research advances in nutritional science (Berg,
1993).
“Malnutrition
is still staggering,” he said, “and in some places, particularly sub-Saharan
Africa, it is getting worse. We of the international nutrition community, I’m
embarrassed to say, have made a disappointingly small dent in improving that
condition.”
The situation has gotten worse over the years
because interest in malnutrition has largely been supplanted by AIDS. As a
consequence, African diseases due to malnutrition are increasingly being listed
as AIDS and consequently treated with toxic drugs.
Over a
decade ago, international organizations had implemented nutritional
interventions for reducing mortality from diarrhea, pneumonia and other common
diseases of malnutrition caused by poverty (Mosley,
1993).
Now, however, the growing practice of treating these diseases as AIDS has
largely replaced and undermined those early efforts (Brewster
et al., 1997).
Indeed, Alex de Waal and Alan Whiteside have even gone so far as to
hypothesize that AIDS is responsible for the present food crisis in southern
Africa (de Waal and Whiteside, 2003). However, a more conventional and convincing
explanation for the worsening malnutrition in southern Africa is the simple
fact that many
Africans lead desperate lives.
According to the Institute
for Democracy in South Africa (Idasa), substantial proportions of all
adults across 15 African countries face at least some shortages of basic
necessities. Over one-half go without enough food to eat at least once a year,
and almost one fifth go without “many times” or “always” (Institute for Democracy in South Africa (Idasa),
2004). Just under
one-half go without enough clean water, and 40% have no toilets. A majority
face shortages of needed medicines or medical treatment. Nearly half go without
enough fuel to cook their food. According to the authors, underlying this
deprivation is Africa’s “unemployment crisis”. Fully three out of four Africans
go without cash income at least once, and over a third do
so frequently.
Confusing malnutrition with AIDS
has contributed to the 50% mortality rates in the hospital-care of severely
malnourished children in the developing world (Nolan et al., 2001; Schofield and
Ashworth, 1996). In sub-Saharan Africa, studies
have shown that 25% of children with malnutrition have antibodies to HIV,
although the patterns of malnutrition are indistinguishable from those who are
HIV-negative (Ball,
1998). A
study of two South African hospitals, for example, found that for 2000-2001,
50% of the deaths of severely malnourished children were due to doctor error
and another 28% to nurse error (Ashworth
et al., 2004). The
authors of the study found that malnutrition was simply not a priority in the
training of the doctors. AIDS so dominates the training and thinking at the
largest teaching hospital in South Africa that diabetes and other common
problems are being misdiagnosed as AIDS (Mhlongo,
2005).
In mid 2006, Sam reported to Mbeki that 90% of seventh-year medical students
across the country cannot diagnose 80% of the diseases and conditions South
Africans suffer because of the over-emphasis on AIDS.
I agree with Andrew Tomkins who said in 2005,
“Now that specific nutrition interventions
have been shown to have beneficial effects, particularly multiple micronutrient
interventions and infant feeding options, governments, development partners,
including various UN agencies, and NGOs need to act” (Tomkins, 2005).
Physician-sponsored
nutritional programs
There were signs
early in 2005 that Mbeki’s opponents would block our proposed full-scale
nutritional clinical trial. As a backup, the Dr. Rath Health Foundation Africa
implemented Physician-sponsored nutritional programs in several communities
throughout South Africa but principally in Khayelitsha,
a township near Cape Town.
Background
Micronutrients play a critical role in the
proper functioning of the immune system. Therefore, it is not surprising that
at the beginning of the AIDS epidemic, researchers began to notice
micronutrient abnormalities in AIDS patients. Chronic diarrhea, anorexia, malabsorption, impaired nutrient storage, increased energy
demands and altered metabolism were the primary contributors to these
nutritional deficiencies (Tang et
al., 2005).
Awareness
of the importance of micronutritients in the
maintenance of a healthy immune system has been increasing as demonstrated by studies of micronutrient
supplementation among antiretroviral drug-naive populations. A series of trials
conducted in Durban, South Africa examined the effects of vitamin A
supplementation on the morbidity and mortality of so-called HIV-infected
mothers and their offspring. Among all children, the supplemented group had a
30% lower overall morbidity (diarrhea, thrush, lower and upper respiratory
tract infections, rash) than the placebo group (Coutsoudis et al., 1995). Between 1995 and 1997, over 1000 so-called
HIV-infected pregnant women in Tanzania were enrolled into a double-blinded,
placebo-controlled micronutrient supplementation trial that
continued through lactation. Multivitamin supplementation, but not vitamin A,
was significantly associated with improved birth outcomes and improvements in
CD4 and CD8 cell counts among these women (Fawzi et al., 1998).
Other studies have shown that providing
pregnant women with multivitamins resulted in higher birth weight (Fawzi et al., 2000), reduced
mortality and progression of disease among children (Fawzi et al., 2002) and
their mothers (Fawzi et al., 2004), and
decreased risk of infant diarrhea (Fawzi et al., 2003). The
disease-preventing and life-preserving effects of micronutrients have been
demonstrated in adults as well (Jiamton et al., 2003).
Below is
documented the extensive clinical benefits from a short-course of
micronutrients (specific vitamins, amino acids, minerals and polyphenol extracts from green tea) administered by
physicians to so-called HIV-positive residents of Khayelitsha
who have never used antiretroviral drugs.
Enrollment
of patients
The people of Khayelitsha display a spectrum of diseases associated with
poverty and malnutrition that overlaps substantially with the Bangui definition
of AIDS (World
Health Organization, 1986).
According to the Bangui definition, Africans with fever, diarrhea, persistent
cough, weight-loss, and (since the mid 1990s) TB are suffering from AIDS.
Local officials
of the South African
National Civic Organization (SANCO) were responsible for enrolling the 100 patients for the Khayelitsha
nutritional program. Beginning May 11, 2005, people were free to join the
nutritional program if they satisfied the following criteria: be over the age
of 13, not pregnant, test positive for antibodies to HIV, not be on
antiretroviral drugs nor have a history of their use, have clinical diseases
(i.e. CDC stages 2 or 3), likely to survive the two-months of observation as
determined by the examining physician, be willing to comply with the vitamin
regimen and dosage, and sign the waiver-informed consent form.
Upon enrolling,
patients were interviewed and their health history assisted with the aid of a
questionnaire. They were then examined by a licensed South African physician
and treated for specific diseases such as diarrhea, TB, and other common
ailments, with the appropriate standard therapies. Patients were hospitalized
when necessary. The patients were given a four-week supply of pills containing
micronutrients. The dosing was 5 pills three times a day. Patients returned
every four weeks for another medical exam and to pick up a new supply of
micronutrients and packages of food. The patients were interviewed about
changes in their health. The period of formal clinical observation was eight
weeks. After eight weeks, the patients were provided with the micronutrients
free-of-charge for as long as they wanted.
Micronutrients
The combination of micronutrients
consisted of: vitamins (ascorbic acid, Nicotinate, Pantothenate, Thiamine, Riboflavin, Pyridoxine, Cyanocobalamin, Folic Acid, Biotin, Beta-carotene, cholecalciferol, d-alpha-Tocopherol), minerals and trace
elements (Magnesium, Calcium, Potassium, Phosphate, Zinc, Manganese, Copper,
Selenium, Chromium, Molybdenum), amino acids (Taurine, L-Lysine, L-Proline, L-Arginine, L-Carnitine, L-Cysteine, N-Acetylcysteine), and other essential
nutrients (Green Tea Leaf Extract, Bioflavonoids,
Inositol, Coenzyme Q-10).
Clinical
and Nutritional Assessment
Enrollees were
scored from 0-4 (0 normal, 4 severe) for severity of numerous indicators of
health. Among them were the typical AIDS-defining diseases for Africa (De Cock et al., 1991; Weniger et al., 1992; World Health Organization, 1986): fever, diarrhea, cough, weight-loss, TB, and opportunistic
infections. Other physical symptoms were assessed: swollen glands, joint pain,
numbness or tingling in the hands or feet, nausea or vomiting, headache,
bloating, rash, irregular heart beat, pain in mouth (lips or gums), cracks in
lips or mouth, sore tongue, wounds and sores that would not heal, gum bleeding,
loose teeth, eyes burning or itching, eyes sensitive to light, blurred vision,
dry or itchy skin, skin bruises, muscle cramps, cold hands or feet, sweating
without work or exertion, unusual thirst, colds and flues. Indicators of general well-being were recordered:
nervousness, irritation, anxiety, depression, insomnia, loss of
appetite, fatigue, dizziness, memory loss.
Finally,
enrollees were questioned as to the frequency with which they consumed specific
items of food available in Khayelitsha: mielie pap, samp, white bread,
brown bread, sweets, hot chips, rice, noodles, sweet potatoes, fish, chicken,
red meat, pronutro/cereals, lemons, oranges,
tomatoes, bananas, grapes, nuts, green peppers, salads, milk, and apples.
Analysis
of Data
The
results from the questionnaires and clinical findings were compiled and scored
from 0 to 4, where 0 indicated no complaints or symptoms for each indication
and 4 was severe. One-way analysis of variance was performed to generate the
averages, standard deviations and significance values.
Results
Of the
100 people who enrolled, 56 completed all three visits of the 8-week nutritional program sponsored by SANCO that began on
May 11, 2005, in Khayelitsha. In addition to the usual reasons people fail to return for
scheduled doctor appointments was the pressure and intimidation the Treatment
Action Campaign (TAC) put on the enrollees personally to stop taking the
micronutrients.
The
observational phase of the nutritional program ended October 30, 2005. The
results for the 56 enrollees showed that within 4-8 weeks of taking the
micronutrients there was a significant reduction (58% overall) in 16 clinical
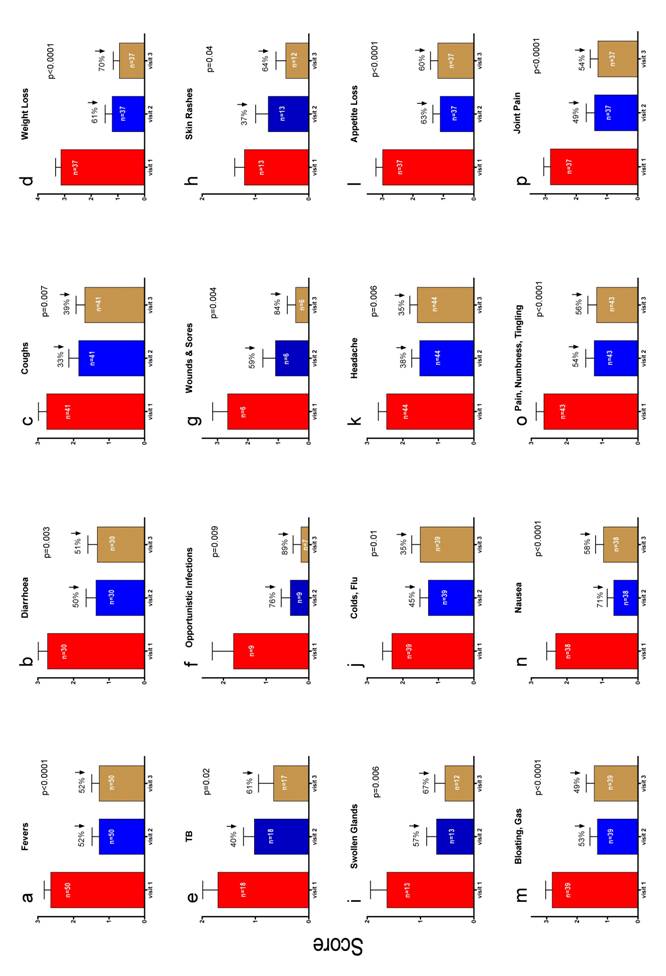
symptoms and conditions (Figure 1). Panels a-f of Figure 2 show there were
rapid and substantial reductions in the AIDS-defining symptoms (De Cock et al., 1991; Weniger et al., 1992; World Health
Organization, 1986). Fevers declined 52%, diarrhoea 51%, coughs
39%, weight-loss 70%, TB 60%, and opportunistic infections 89%. There was
dramatic healing of wounds and sores that had persisted for months prior to
taking the micronutrients (Figure 2g) and skin rashes dramatically improved
(Figure 2h). There was also a significant reduction in swollen glands (Figure
2i).
Conclusion
The
broad-spectrum clinical benefits observed for a short-course of micronutrient
supplementation given to the poor of Khayelitsha township argues powerfully for formal
clinical trials to assess the extent and duration of these benefits. People
with and without antibodies against HIV should be included to determine if
there is a difference between the groups.
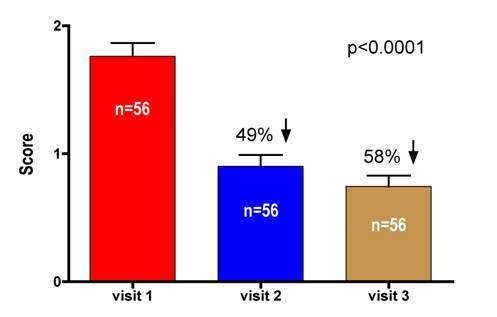
Fig. 1. Overall improvement of 16 clinical symptoms combined during an
8-week course of micronutrient supplementation.
Of the 100 people that enrolled in the micronutrient program, 56 completed all three visits. There was a 49% improvement after only 4 weeks on the micronutrients, that increased to nearly 60% at week 8.
Fig. 2. Improvements in Specific Clinical Symptoms.
(a-f) There were significant reductions in the AIDS-defining
symptoms (Weniger et al., 1992; World Health
Organization, 1986) after only 4 weeks of taking micronutrient supplementation. Fevers
declined 52%, diarrhoea 51%, coughs 39%, weight-loss
70%, TB 60%, and opportunistic infections 89%. (g) There was dramatic healing
of wounds and sores that had persisted for months prior to taking the
micronutrients. (h) Skin rashes dramatically improved. (i)
There was also a significant reduction in swollen glands.
References
Ashworth,
A., Chopra, M., McCoy, D., Sanders, D., Jackson, D., Karaolis,
N., Sogaula, N., and Schofield, C., 2004. WHO
guidelines for management of severe malnutrition in rural South African
hospitals: effect on case fatality and the influence of operational factors. Lancet 363, 1110-5.
Ball, C.S., 1998. Global issues in pediatric nutrition: AIDS. Nutrition 14, 767-70.
Berg, A., 1993. Sliding toward nutrition
malpractice: time to reconsider and redeploy. Am
J Clin Nutr 57, 3-7.
Brewster, D.R., Manary, M.J., and Graham,
S.M., 1997. Case management of kwashiorkor: an intervention project at seven
nutrition rehabilitation centres in Malawi. Eur J Clin Nutr 51, 139-47.
Coutsoudis, A., Bobat, R.A., Coovadia, H.M.,
Kuhn, L., Tsai, W.Y., and Stein, Z.A., 1995. The effects of
vitamin A supplementation on the morbidity of children born to HIV-infected
women. Am J Public Health 85, 1076-81.
De Cock, K.M., Selik, R.M., Soro, B., Gayle, H., and Colebunders,
R.L., 1991. For debate. AIDS surveillance
in Africa: a reappraisal of case definitions. Br Med J
303, 1185-8.
de Waal, A., and Whiteside, A., 2003. New variant famine: AIDS
and food crisis in southern Africa. Lancet 362, 1234-7.
Department of Health, SA Clinical trial information, South African
National Clinical Trial Register, 2008,
http://www.sanctr.gov.za/SAClinicalTrials/tabid/169/Default.aspx.
Fawzi, W.W., Msamanga, G.I., Wei, R., Spiegelman, D., Antelman, G., Villamor, E., Manji, K., and
Hunter, D., 2003. Effect of providing vitamin supplements to
human immunodeficiency virus-infected, lactating mothers on the child's
morbidity and CD4+ cell counts. Clin Infect Dis 36, 1053-62.
Fawzi, W.W., Msamanga, G.I.,
Hunter, D., Renjifo, B., Antelman,
G., Bang, H., Manji, K., Kapiga,
S., Mwakagile, D., Essex, M., and Spiegelman,
D., 2002. Randomized trial of vitamin
supplements in relation to transmission of HIV-1 through breastfeeding and
early child mortality. Aids 16, 1935-44.
Fawzi, W.W., Msamanga, G.I., Spiegelman, D., Wei, R., Kapiga, S., Villamor, E., Mwakagile, D., Mugusi, F., Hertzmark, E., Essex, M., and Hunter, D.J., 2004. A randomized trial of multivitamin supplements
and HIV disease progression and mortality. N Engl
J Med 351, 23-32.
Fawzi, W.W., Msamanga, G.I., Spiegelman, D., Urassa, E.J.,
McGrath, N., Mwakagile, D., Antelman,
G., Mbise, R., Herrera, G., Kapiga,
S., Willett, W., and Hunter, D.J., 1998. Randomised trial of effects of vitamin supplements on
pregnancy outcomes and T cell counts in HIV-1-infected women in Tanzania.
Lancet 351, 1477-82.
Fawzi, W.W., Msamanga, G.,
Hunter, D., Urassa, E., Renjifo,
B., Mwakagile, D., Hertzmark,
E., Coley, J., Garland, M., Kapiga, S., Antelman, G., Essex, M., and Spiegelman,
D., 2000. Randomized trial of vitamin
supplements in relation to vertical transmission of HIV-1 in Tanzania. JAIDS 23, 246-54.
Institute for Democracy in South Africa (Idasa), Lived Poverty in Africa:
Desperation, Hope and Patience, Afrobarometer
2004, www.afrobarometer.org
Jiamton, S., Pepin, J., Suttent,
R., Filteau, S., Mahakkanukrauh,
B., Hanshaoworakul, W., Chaisilwattana,
P., Suthipinittharm, P., Shetty,
P., and Jaffar, S., 2003. A randomized trial of the impact of multiple micronutrient supplementation on mortality among HIV-infected individuals
living in Bangkok. Aids 17, 2461-9.
Mhlongo, S., Diabetes misdiagnosed as AIDS in the teaching hospital
at the University of Limpopo, MEDUNSA campus (personal communication), 2005,
Mosley, W., 1993.
Disease control priorities in developing countries. World
Bank through Oxford University Press, New York.
Nolan, T., Angos, P., Cunha,
A.J., Muhe, L., Qazi, S., Simoes, E.A., Tamburlini, G.,
Weber, M., and Pierce, N.F., 2001. Quality of hospital care
for seriously ill children in less-developed countries. Lancet 357, 106-10.
Piot, P., The
first line of defense, World Food Program: why food and nutrition matter in the
fight against HIV/AIDS,
United Nations, Rome 2003,
http://www.wfp.org/policies/Introduction/other/index.asp?section=68sub_setion=1#.
Schofield, C., and Ashworth, A., 1996. Why have mortality rates for
severe malnutrition remained so high? Bull World Health Organ 74, 223-9.
Tang, A.M., Lanzillotti, J., Hendricks,
K., Gerrior, J., Ghosh, M.,
Woods, M., and Wanke, C., 2005. Micronutrients:
current issues for HIV care providers. Aids 19, 847-61.
Tomkins, A.M.,
2005. Evidence-based nutrition interventions for the control
of HIV/AIDS. S African J Clin Nutri 18, 187-191.
Weniger, B.G., Quinhoes, E.P., Sereno, A.B., de
Perez, M.A., Krebs, J.W., Ismael, C., Sion, F.S., Ramos-Filho, C.F., de
Sa, C.A., Byers, R.H., and et al., 1992. A simplified
surveillance case definition of AIDS derived from empirical clinical data. The
Clinical AIDS Study Group, and the Working Group on
AIDS case definition. JAIDS 5, 1212-23.
World Health Organization, 1986. Provisional WHO clinical case definition for
AIDS. Weekly Epidemiological Records March, 7, (10), 72-73.